

BY: Dr. Farhat Naz

Face of patient with Achondroplasia

Adnan a 26 years old male with dwarfism presented with history of fever and shortness of breath for the last one month. Fever was high grade, intermittent and relieved with panadol. He also complains of shortness of breath which is there for the last few months. The shortness of breath is mild and felt more on lying down.
There is no headache, sore throat and abdominal pain but there is increase frequency and burning of urine for last few days and abdomen is swollen for last one month.
past History:
He is a special child since birth and born with short stature which became more evident after the age of 5 years and he could not attend the school and receive formal education. He has recieved some education at home but cannot write. He had normal memory and intelligence and did not have movement disability. He had fracture of left thigh three years back after which he is unable to walk. He did not have any major illness in past but was investigated for shortness of breath 3 years ago and was diagnosed with heart problem for which he recieved treatment.
He was also hospitalized one month back for fever and got treated for urinary tract infection.
Family history:
His parents are normal and rest of elder members of family are normal both on maternal and paternal sides. He has 9 siblings out of which four other siblings were dwarf including 2 brothers and 2 sisters. His all dwarf siblings died between the ages of 16-25 years and he is the only one left with disability.
Apart from dwarfism, his father is hypertensive. There is no history of any other significant disease in family.
Drug history:
He is taking medications for his cardiac problem including frusamide and aldactone.
Personal history:
He is unmarried person with happy mood and normal sleep and bowel habits. There is no addiction. He can perform his routine activities and not dependant on others for eating and clothing but he is unable to walk for last three years after having leg fracture, and needs family support.
Socioeconomic history:
He belongs to a poor background and cannot afford the treatment in hospital. His father is jobless and family is dependent on earning of brother.
Pysical Examination:
A dwarf patient with mature facial appearance sitting in the bed. The head appears large and nasal bridge appears flattened. There is no pallor, jaundice or cyanosis.
B.P. 120/70mmHg, pulse: 104/min, regular, temp 100F, Respiratory rate: 18/min
On neck examination: neck vein are prominent with prominent Carotid pulsation and raised JVP. There is no lypmhadenopathy and no peripheral odema but having mild sacral odema.
Muskoloskeletal examination:

Short stature with short arms and legs, Malformed forearms, thighs, hands and feet. Fingers and toes are small, there is increased curvature of feet with bent fingers.
The chest is pigeon shaped and spine is curved posteriorly (kyphosis) and increased lumbar lordosis.
Cardivasular:
The heart is enlarged with laterally displaced apex beat. The second heart is louder at apex. There is pansystolic murmur at mitral area and early diastolic murmur at aortic area suggestive of aoric and mitral regurgitation.
Respiratory:
Respiratory rate is normal. Air entry is equal in both lungs with normal vesicular breathing and mild end inspiratory crackles.
Abdomen:
Abdomen is distended with flattend umbilicus and fullness in flanks. There is mild enlargement of liver and shifting duĺlness and fluid thrill are positive suggesting moderate ascites.
Neurological:
Patient is consious, oriented with normal mood and orientation. There is no neurological deficit on examination.
Investigations:
Investigations are suggestive of urinary tract infection. C Reactive Protein and White cells count are raised but rest of septic profile including d-dimers, PT, APTT, serum ferritin are normal.
Echocardiography:
Left ventricular Ejection Fraction: 40%, moderatre Mitral and moderate aortic regurgitation suggestive of cardiac failure secondary to rheumatic heart disease.
What is Achondroplasia?
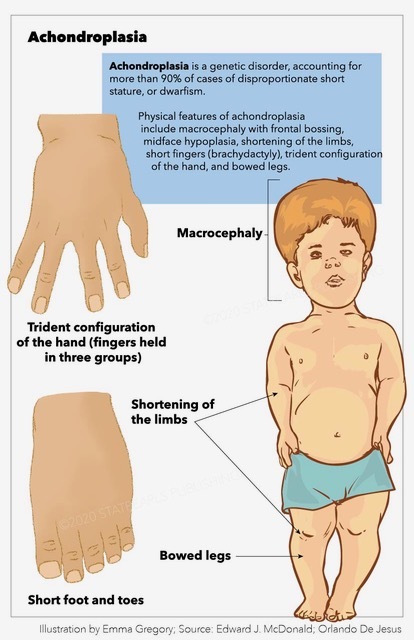
Achondroplasia, a genetic disorder affecting bone growth, stands as the most common form of short-limbed dwarfism. This condition, characterized by disproportionate short stature, emerges from a genetic mutation that impacts the development of the bones.
Epidemiology:
Achondroplasia is a rare disorder, with an estimated prevalence of 1 in 15,000 to 40,000 live births. It affects all ethnic groups equally and occurs sporadically, often without a family history. Advanced paternal age is associated with an increased risk of having a child with achondroplasia.
Definition:
Achondroplasia’s name is derived from the Greek words “a-” (without), “chondro-” (cartilage), and “-plasia” (formation). Essentially, it signifies the incomplete formation of cartilage, leading to abnormal bone growth.
Inheritance:
This condition follows an autosomal dominant pattern of inheritance. The majority of individuals with achondroplasia have parents of average height, and the mutation occurs spontaneously during sperm or egg formation. Offspring of an affected individual have a 50% chance of inheriting the mutated gene.
Gene locus of achondroplasia:
Achondroplasia is primarily associated with a mutation in the fibroblast growth factor receptor 3 (FGFR3) gene. The FGFR3 gene is located on the short arm of chromosome 4 at position 4p16.3. This specific gene mutation results in the abnormal production of the FGFR3 protein, a receptor involved in regulating bone growth and development.
The specific mutation responsible for achondroplasia involves a single nucleotide change in the FGFR3 gene, leading to the substitution of glycine for arginine at position 380 (Gly380Arg). This genetic alteration disrupts the normal functioning of the FGFR3 protein, ultimately affecting the regulation of bone growth and contributing to the characteristic features of achondroplasia.
Clinical Features:
The hallmark feature of achondroplasia is short stature, typically below the average height for one’s age. The limbs are disproportionately short compared to the trunk, and the fingers are short and stubby. The head is usually large with a prominent forehead and a flattened bridge of the nose. Other common features include a prominent lumbar lordosis, limited elbow extension, and bowed legs.
Challenges in Adults with Achondroplasia:
While achondroplasia is often diagnosed in childhood, individuals face unique challenges as they transition into adulthood. Orthopedic issues such as back pain, joint problems, and spinal stenosis become more prominent. Social challenges related to employment, relationships, and societal perceptions may also impact the quality of life for adults with achondroplasia.
Life Expectancy:
Historically, individuals with achondroplasia faced a reduced life expectancy due to complications related to spinal compression and respiratory issues. However, with advancements in medical care and management strategies, life expectancy has improved. Many individuals with achondroplasia now live into their 60s and beyond.
Cause of Death:
The most common cause of premature death in individuals with achondroplasia is often related to neurological and respiratory complications. Spinal stenosis, a narrowing of the spinal canal, can lead to compression of the spinal cord, resulting in neurological deficits. Respiratory issues, such as sleep apnea and restrictive lung disease, may contribute to complications that can impact life expectancy.
Achondroplasia and cardiac problems:
While achondroplasia primarily affects bone growth, it can have implications for other organ systems, including the cardiovascular system. Individuals with achondroplasia may experience certain cardiac issues, although these are not as common or pronounced as the orthopedic challenges associated with the condition.
One notable concern is the potential for hydrocephalus (accumulation of fluid in the brain) in infants with achondroplasia, which can indirectly impact cardiac function. Increased intracranial pressure can lead to cardiac changes and compromise overall cardiovascular health.
Additionally, there may be cardiovascular considerations in the broader context of managing achondroplasia:
Reduced Exercise Tolerance:
The physical characteristics of achondroplasia, such as short limbs and stature, may contribute to reduced exercise tolerance. Engaging in regular physical activity is crucial for cardiovascular health, so individuals with achondroplasia may need to find suitable, low- impact activities to maintain cardiovascular fitness.
Respiratory Impact:
Respiratory issues, common in individuals with achondroplasia, can indirectly affect the cardiovascular system.
Conditions like sleep apnea, which are prevalent in this population, may lead to intermittent drops in blood oxygen saturation potentially impacting the heart over time.
Cardiac Screening:
While not a routine aspect of achondroplasia management, some healthcare providers may consider periodic cardiac screening, especially if there are additional risk factors or symptoms present. This can involve monitoring blood pressure, assessing heart function, and evaluating cardiovascular risk factors.
Anesthetic Considerations:
During surgical procedures or medical interventions, anesthesiologists need to consider the unique anatomy of individuals with achondroplasia. Proper precautions are taken to minimize the risk of complications, including those related to the cardiovascular system.
It’s important to note that cardiac problems in achondroplasia are not a universal feature, and many individuals with this condition do not experience significant cardiovascular issues. Regular medical check-ups and a comprehensive healthcare approach, involving specialists familiar with achondroplasia, can help address potential concerns and ensure overall well-being. As research and clinical understanding of achondroplasia continue to advance, further insights into potential cardiac implications may emerge, influencing both diagnosis and management strategies.
Diagnosis:
Achondroplasia is often diagnosed through clinical examination and confirmed by genetic testing. Prenatal diagnosis is possible through molecular genetic testing of DNA obtained by chorionic villus sampling or amniocentesis.
Management:
The management of achondroplasia is multifaceted and involves a collaborative approach between various medical specialties. Early intervention and comprehensive care are crucial for optimizing outcomes.
Orthopedic Interventions: Orthopedic management focuses on addressing skeletal abnormalities and preventing complications. Limb- lengthening procedures, spinal decompression surgeries, and joint interventions may be considered based on individual needs.
Respiratory Support: Given the predisposition to respiratory issues, regular monitoring and early intervention for conditions like sleep apnea are essential. Continuous positive airway pressure (CPAP) therapy is often employed to improve breathing during sleep.
Physical Therapy: Physical therapy plays a vital role in enhancing mobility, strength, and overall physical well-being. Tailored exercise regimens can help manage joint stiffness and improve flexibility.
Genetic Counseling: Individuals and families affected by achondroplasia benefit from genetic counseling, providing information about the condition, inheritance patterns, and family planning options.
Psychosocial Support: Addressing the psychosocial aspects of living with achondroplasia is crucial. Support groups, counseling, and educational resources contribute to the well-being of individuals and their families.
In conclusion, achondroplasia presents both medical and psychosocial challenges across the lifespan. As our understanding of the genetic basis and clinical management of this condition continues to evolve, so too does the potential for improved outcomes and enhanced quality of life for those affected. A comprehensive and collaborative approach, involving medical professionals, genetic counselors, and supportive communities, is essential for navigating the complexities associated with achondroplasia.
